After one month of escalated bombardment and blanket evacuation orders by Israeli forces in Lebanon, more than one million people have been forcibly displaced. Among the most vulnerable are migrant workers from different African and Southeast Asian countries and other minorities, increasingly cut off from humanitarian assistance.
Struggling to afford medical care and navigate restrictive legal systems, displaced migrant communities are now trapped between the impacts of war and a humanitarian response that often excludes them. The International Organization for Migration (IOM, 26 March 2026) estimates that 48,000 of those displaced or living in high-risk areas are migrants, representing around 30 percent of the identified migrant population in Lebanon (IOM, 2025).
In Beirut, Médecins Sans Frontières (MSF) had been providing care through its Bourj Hammoud clinic, a northern suburb of Beirut, provided around 1,500 consultations of medical care, mental health support and social services a month. In response to the growing needs following Israel’s escalation of attacks, MSF has expanded through its mobile clinics reaching forcibly displaced communities across the city and surrounding areas. Together, the clinic and two mobile clinics are now providing some 3,000 consultations per month, as well as distribution of core relief items and food support to migrant-led community kitchens.
Since early March, medical referrals from MSF’s Bourj Hammoud clinic have doubled, with many patients requiring blood transfusions, intensive care admissions, or surgery. This increase reflects both the escalation of the war and the suspension of the International Organization for Migration referral programme in January. Other actors are also struggling to fill these gaps due to lack of funding, leaving many patients without access to lifesaving care.
I was living in Dahiyeh (Beirut's southern suburbs) when the bombardment started. We fled that same night, not knowing where to go. We ended up on the road, searching for shelter, knocking on doors that wouldn’t open, asking for help that never came. There was nowhere for us. No safety. Just the road beneath us.
Salam
Displaced Migrant
Migrant communities in Lebanon already face significant economic, legal and social barriers to accessing basic services. Many are now sheltering in overcrowded accommodations arranged by community leads, or sleeping on the streets, with some reportedly being explicitly turned away, discriminated against, or deprioritized from formal collective shelters in favour of Lebanese nationals.
Even before Israel’s latest military escalation in Lebanon, migrants’ access to healthcare was severely limited by language barriers, systematic discrimination, cost of health services and residency status. Now, with nearly a fifth of the country’s population forcibly displaced, migrants are becoming even more pushed to the sidelines, with devastating consequences to their health and survival.
AbdelHalim Abdallah
MSF project coordinator in Beirut
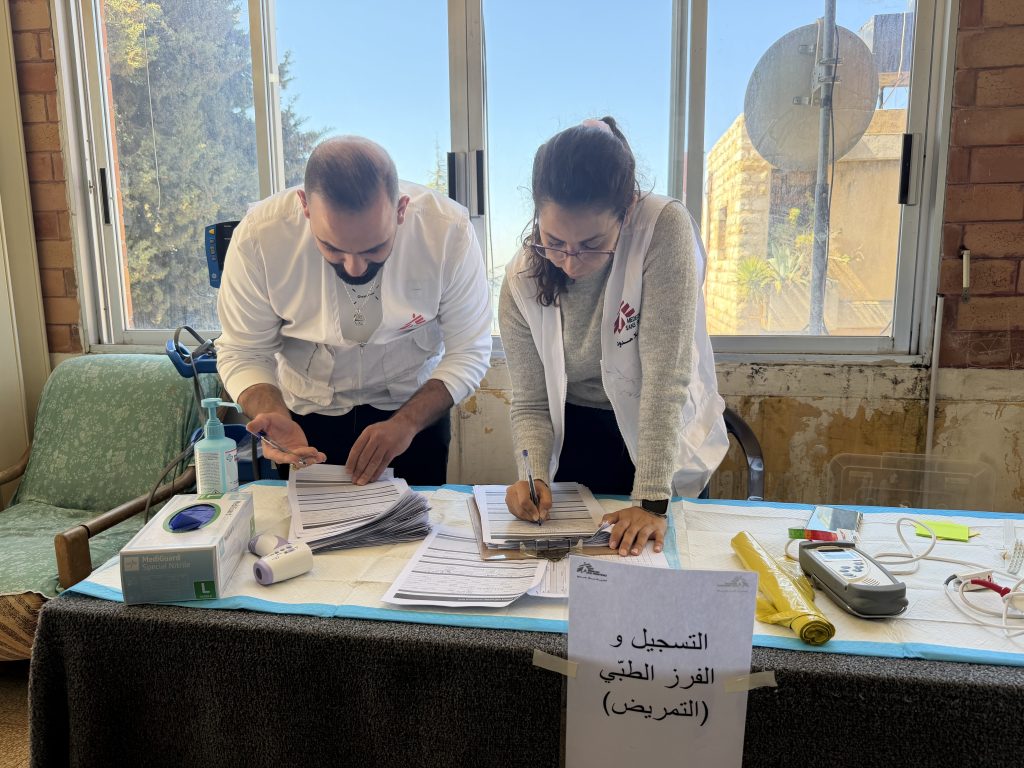
On the last Sunday or March, MSF treated over 300 migrant patients in its Bourj Hammoud clinic and two mobile clinic locations in Beirut and Saida. Over 170 patients from Ethiopia and Bangladesh sought MSF’s healthcare services in Saida alone. Most of them were either displaced or haven’t had access to healthcare for months. The team had to send two babies that day to the emergency room. The patients just kept on coming.
While families are left homeless and displaced, their health needs are also exacerbated due to disruptions to care, high costs of medicine, and lack of access to care due to irregular residency status. Although access to care has been severely constrained for migrant communities in the past, it’s become even more challenging as the needs across the country have dramatically grown.
Around one quarter of the medical consultations provided by MSF mobile clinic teams treating migrant communities are for chronic illnesses, with many patients having been cut off from their medication due to forced displacement or other barriers to accessing healthcare. MSF teams are also observing significant gaps in people’s access to women’s healthcare and mental health services, even where primary healthcare is being provided by other actors.
MSF teams have scaled up their response to meet the growing needs of forcibly displaced people in Lebanon including migrants and other minorities. Yet, these communities remain underrepresented in the nationwide humanitarian response led by international actors and the government. As a result, many continue to rely on community-led initiatives, which are often unable to address more complex needs such as medical or psychological ones.
Migrant workers, who majorly come from Ethiopia, Bangladesh, and Sri Lanka to do domestic and other blue-collar work, have been systematically marginalised under Lebanon’s Kafala (sponsorship) system that grants them minimal rights, including health coverage. They have also been excluded from previous humanitarian response to the country’s previous crises.
MSF response
MSF has been providing specialised care for migrant communities since 2019 through the support of volunteer community health educators who speak Amharic, Bangla, Sinhala, French, English, and Arabic. These volunteers ensure that migrant patients can communicate with our healthcare professionals.
Since 2024, MSF’s clinic in Bourj Hammoud, a northern suburb of Beirut, has been providing primary health care, mental health support, sexual and reproductive care, social services as well as health promotion.
To scale up our response to the current escalation, the clinic is now open 6 days per week, runs two mobile medical units covering the needs of migrant workers across the country as well as displaced Lebanese families in over 20 locations in neighbouring districts in Mount Lebanon. Additionally, the clinic supports eight local community kitchens with raw materials to prepare about 1,000 meals a day, who deliver them to both displaced migrants as well as those still living in high-risk areas and areas under blanket evacuation orders.
Across Lebanon, including in high-risk areas, MSF teams has distributed over 2,000 core relief items, including blankets, mattresses and hygiene kits to over 100 migrant community houses and shelters.
Like many websites, MSF uses cookies to enhance your user experience. By continuing to navigate this site you are giving consent to the issue of these cookies. No, give me more info
This website uses cookies to improve your experience while you navigate through the website. Out of these cookies, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may have an effect on your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. This category only includes cookies that ensures basic functionalities and security features of the website. These cookies do not store any personal information.
Any cookies that may not be particularly necessary for the website to function and is used specifically to collect user personal data via analytics, ads, other embedded contents are termed as non-necessary cookies. It is mandatory to procure user consent prior to running these cookies on your website.