COVID-19 stresses led to a spike in violence for people living with their abusers
In March 2020, to curb the spread of COVID-19, India joined several other countries around the world in imposing strict lockdown measures and redirecting health resources to meet the needs arising from the pandemic. Globally, such measures resulted in limited access to sexual and reproductive health care including safe abortion, contraception, and treatment for sexual violence. A tragic consequence of these restrictions is that an unknown number of people living with their abusers were suddenly trapped, with no access to treatment and no way to escape.
At the height of the pandemic’s first wave, a clinic run by Doctors Without Borders/Médecins Sans Frontières (MSF) in India’s capital, New Delhi, was the only place for a population of nearly a million people to receive treatment for sexual and gender-based violence (SGBV). According to those who work with survivors, however, the biggest impediment to connecting people with care was the breakdown in community outreach. This crisis helped crystallize the fact that no progress can be made against SGBV without engaged and sustained community interaction. Once outreach was allowed to resume, MSF’s clinic saw a shocking three-fold increase in patients.

Crucial community connections
MSF’s SGBV clinic sits on a highly trafficked main road in Delhi’s Jahangirpuri neighbourhood, a densely populated, low-income area. Here, intimate partner violence (IPV) — physical, sexual, or psychological harm that’s inflicted by a spouse or another intimate partner—is the most common type of abuse the clinic staff encounter.
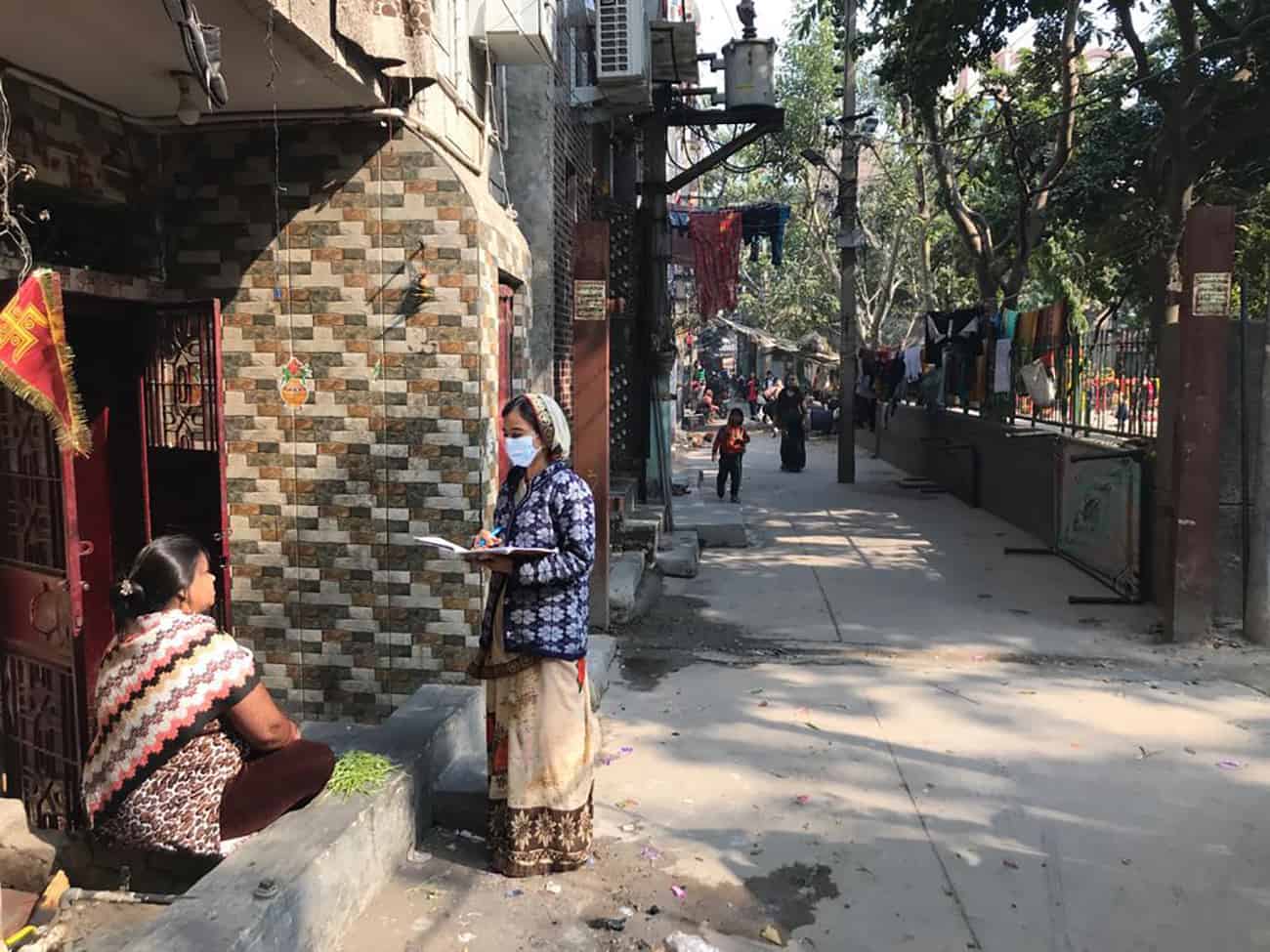
Poonam Devi and Pooja* are part of the SGBV clinic’s active outreach team that goes into the community to raise awareness about sexual violence and bring those who need care into the clinic. Nearly every survivor who comes to the clinic is there because they were persuaded by dedicated workers like Poonam and Pooja. But identifying and building trust with people who’ve been abused and isolated is extremely challenging, and in a place like Jahangirpuri it requires a network of connections. Much of the team’s effectiveness depends on creating and maintaining relationships with grassroots nongovernmental organizations (NGOs) and volunteer Accredited Social Health Activists (ASHAs).
“As ASHAs, our mandate is health, but there are a lot of related issues that come up and influence health-seeking behavior [such as domestic violence] and we have to address them,” says Seema Rani, a volunteer with India’s National Health Mission and with MSF. The ASHAs [Asha means “hope” in Hindi] are community health workers with a long list of responsibilities that includes a special focus on sexual and reproductive health and newborn and child health. They are fixtures in the areas they are assigned to, so they know the community and the community knows them.
Members of the outreach team regularly join the ASHAs on their rounds, and ASHAs connect them with people in the community who need the services that UKK clinic provides—post-exposure prophylaxis (PEP) to protect survivors from HIV, testing for HIV and other sexually transmitted diseases, contraception, safe abortion care in the first 12 weeks, wound care, mental health counseling, and more.
Lockdowns exacerbate domestic violence and limit access to care
When the coronavirus pandemic hit Delhi, Seema and the seven other ASHAs who volunteer with MSF were instructed by the National Health Mission to turn their focus to COVID-19 activities—conducting screenings and helping to initiate contact tracing. When this happened, “there was chaos in the community,” she says.
“Women didn’t have as much access to the ASHA workers and the information and access we would normally give them related to family planning, because we were so busy with COVID,” Seema says. “During the lockdown, the number of unwanted pregnancies in the community increased substantially.”
The SGBV clinic staff members were also limited in what they could do. They tried reaching out to existing patients by phone, but there were issues with that. Survivors frequently don’t have their own phones—they share one with the rest of the family — so they often missed the clinic’s calls. It was also difficult for them to feel comfortable speaking about their situation while trapped at home with family members.

While connecting with existing patients was challenging, reaching new patients was impossible. “We couldn’t go into the community, and we couldn’t meet new people over the phone,” says Poonam. “So that left a huge gap where we were trying to connect the community with the clinic’s services.”
“The NGOs we work with were struggling to operate,” says Pooja. “During this period, we lost some of our connections as people left and new people came to Jahangirpuri who we didn’t know, and that made it hard to continue the relationships.” The area is home to many migrant workers from across India.
Meanwhile, the lockdown was exacerbating the violence. Perpetrators were spending more time at home and many had lost their jobs, creating both social isolation and economic stress, factors that are known to stoke domestic abuse. “The violence had increased, definitely,” says Dr. Geetika Singhal, a physician at SGBV clinic, “but survivors were not able to come out and seek help for it.”
This situation is not unique to India. According to UN Women, reports and calls to helplines for domestic violence in countries including France, Italy, Singapore, and Peru have spiked during lockdown periods. Many policy decisions around the world deprioritized access to care for victims of sexual and gender-based violence, despite the widely known fact that crises often lead to an increase in violence against women and children.
Besides the SGBV clinic, all the other hospitals and clinics in the Jahangirpuri area that offer treatment for sexual violence closed those services in order to redirect their resources to the needs of COVID-19 patients. Shelters for survivors who needed a safe space were not functioning, nor were the courts to provide a legal means of protection.
A survivor who sought help from the SGBV clinic to file for divorce was not able to do so because the courts were not open, and the legal services that would ordinarily help women navigate the system were unavailable. What that woman experienced during the lockdown was similar to what other survivors were facing, says mental health counselor and educator Divya Batra. “[The husband] was very frustrated, he was also drunk, and all that anger and all that frustration were coming out on this woman and her child. So the situation was really difficult for her during those two and a half months of the strict lockdown.” Eventually, she was able to file for divorce and he moved out.

The pace of progress
The UKK clinic was conceived as a model of effective treatment for SGBV survivors—open 24 hours, seven days a week—that could be replicated across India. The idea for the program was spurred by the Nirbhaya case, a horrific attack in which a 23-year-old medical student was gang raped, beaten, and tortured by six men on a bus, and later died from her injuries. The crime, which occurred in December 2012, received international media attention and triggered a storm of protests about the prevalence of violence against women in India. In March 2020, four of the men convicted of gang rape and murder were executed by the state, but the news was largely buried amid concerns over the pandemic lockdown.
Over the last eight years, the Nirbhaya case and others like it across India have increased awareness of how widespread sexual violence is, says Divya, but there is still a long way to go. “The blame or the responsibility is still more on the survivor than the perpetrator themselves,” she says. “That is still the key notion that is there.”
When the lockdown order was eased in May, Seema and the other ASHAs began bringing survivors to MSF’s SGBV clinic again—and in record numbers. By summer, the clinic was seeing three times as many people coming for treatment.
Poonam and Pooja began re-establishing relationships with the NGOs, introducing themselves to new case managers and explaining what MSF is and what services the SGBV clinic offers, so they could start collaborating again.
The clinic was facing an increased need and the same difficult challenges.
“The main issue with survivors of intimate partner violence is that they are not able to leave their partners, so they are chronic survivors,” says Dr. Geetika. “Even if we give them medicines for gonorrhea or chlamydia, for example, and treat their injuries, they are going back to the same person.” A month later, they might come back with the same problems, she says. “I think it’s really tough on these women, and we also feel helpless at times because the cycle—it just goes on and on.”
“If you look at intimate partner violence, the concrete and obvious solution would be, okay, so you leave the marriage and then your problem may be solved,” says Divya. “But that is not an option with the majority of the women that we see.” Most of them are financially dependent on their husbands, which is a major barrier, she says. Since many of them are migrants, they are not very familiar with the area or the rest of the community. And they often have little or no support from the people closest to them because violent behaviors and suffering have become normalized.
Complaining about it carries a lot of stigma and is not encouraged in the country’s laws. “Indian law doesn’t recognize marital rape as a crime,” Divya says, “so that gives the sense that it’s not something we should see as wrong.”
Globally, at least 60 percent of women who experience sexual violence of any kind never report it, according to UN Women. The factors that make SGBV such a difficult crime to report and seek care for—including fear, shame, and stigma—are stark for survivors of intimate partner violence, reducing the likelihood that they will leave an abusive partner. “They’ve accepted that this is their reality and don’t see the violence as something they need to get away from. But, that’s where the outreach team comes in,” Divya says. “They will tell them there is a solution outside of living like this, and there is a way you can come out of it.”

“The first person a survivor of intimate partner violence is going to go to is a family member or friend,” says Pooja, who spends a lot of time talking one-on-one with people in the community. Unfortunately, survivors often don’t get any support from the people closest to them, she says. Instead, they are told to go back to their abuser—they might even be mocked for complaining about it. “And if their family members don’t understand, why would they think a clinic or someone they don’t even know from the outside would be able to help? This is why establishing trust is one of the major things we work on.”
MSF has been able to build trust within communities by collaborating with grassroots NGOs that have a special focus, like support for transgender people or sex workers, and working alongside the ASHAs. These connections help many more survivors receive treatment and, hopefully, start considering how to leave the abusive, unhealthy, possibly life-threatening, situations they are trapped in.
“Before the MSF project was here,” says Seema, one of the ASHA volunteers, “we would refer sexual violence survivors to the government hospitals, but they usually didn’t feel comfortable going there. Now that we are working with MSF, the level of trust we have with the community has even deepened and strengthened because of the kind of treatment MSF provides.”
Perhaps what most distinguishes MSF’s care from that of other providers in the area is the focus on confidentiality. Patients’ names are not used in front of others, their stories are heard in private, and they are not asked to repeat their testimonies multiple times. Staff members at every level are trained to respect the privacy of anyone who comes to the clinic. These considerations are not usually observed in the government hospitals.
“That is, I think, what helps [patients] and what gives some of them this assurance that, yes, this is something that I can trust, and this is something that I can go back to,” Divya says.
* Last name withheld for privacy
Read more about the Umeed Ki Kiran clinic here.









