MSF Scientific Day Asia 2025 will feature a new Exhibition Component to bring a humanistic perspective to the event. Through narratives, photographs, videos, and photovoice, this exhibition will showcase selected abstracts in an experiential and impactful format, highlighting the lived realities behind the data.
By combining storytelling and art, the exhibition seeks to inspire action on pressing health issues, amplify patient voices, and bridge the gap between science, policy, and humanity. This initiative reaffirms MSF’s commitment to community-led action and equitable healthcare solutions.
Exhibitions
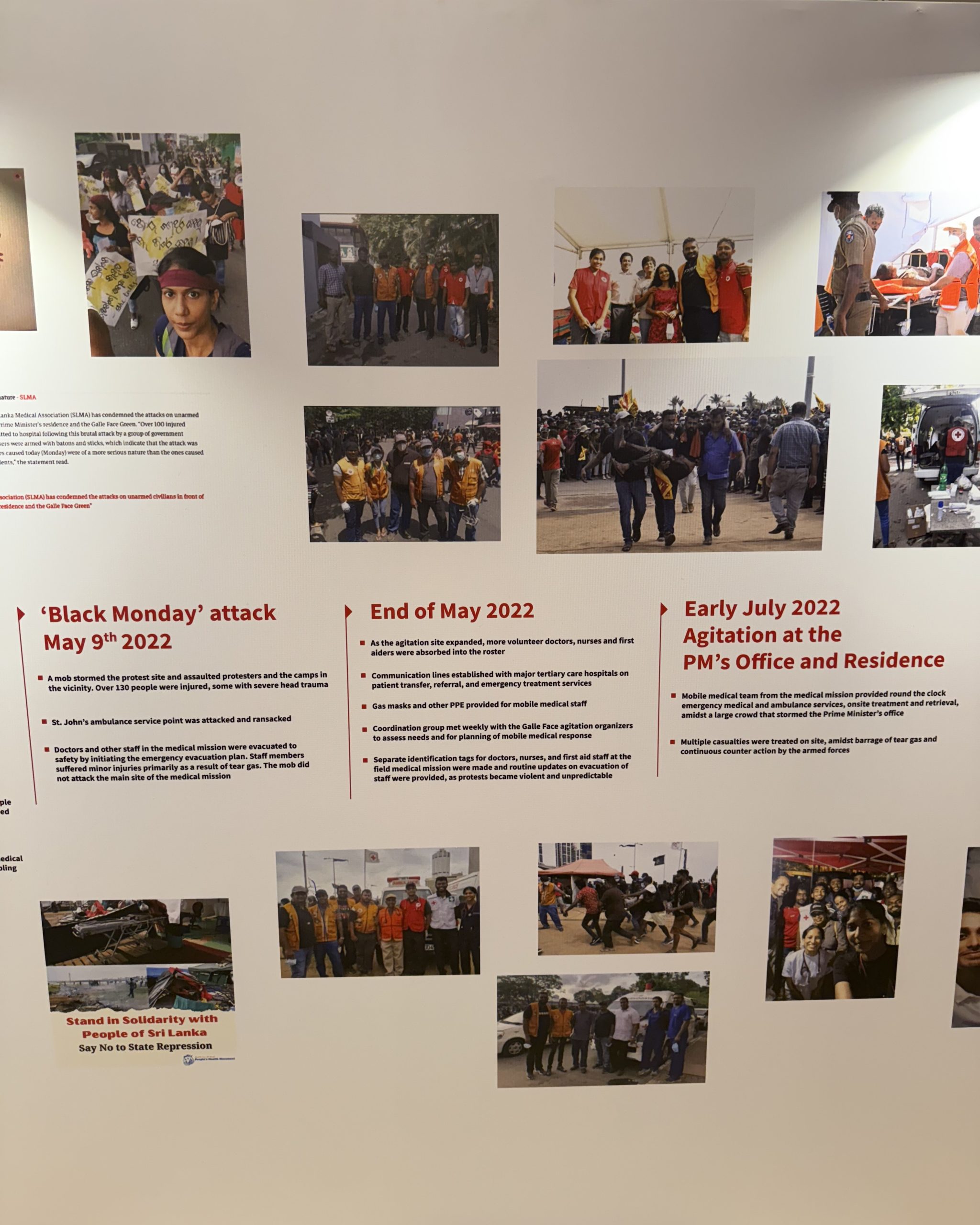
Sanity amidst chaos: The curious case of the ‘Áragalaya’ street medics
V. Ariyaratne, Sarvodaya Shramadana Movement of Sri Lanka & U. Fernando, Uppsala University, Uppsala, Sweden
Introduction
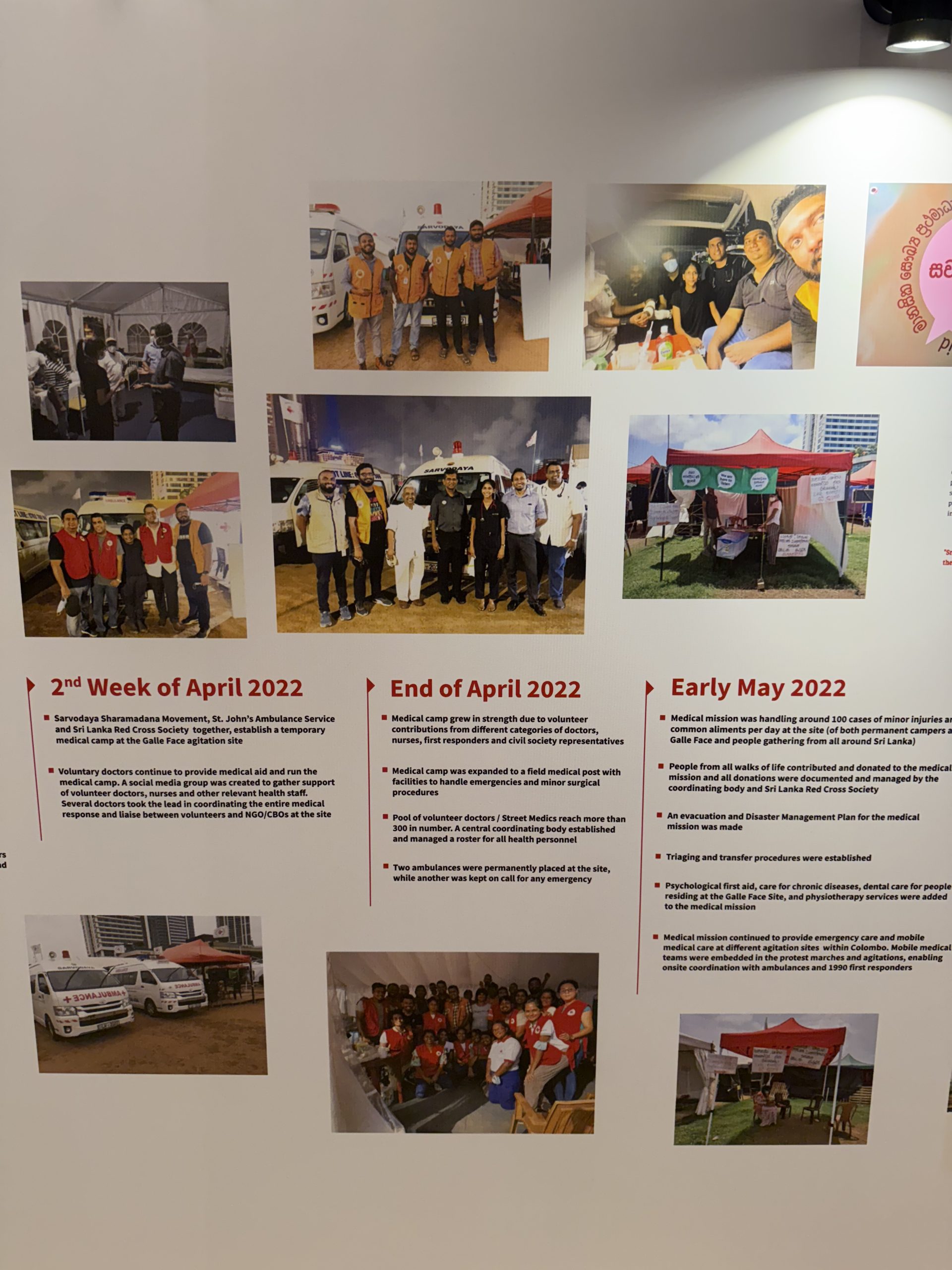
As Sri Lanka plunged into chaos and civil strife (Aragalaya) in early April 2022, several concerned doctors and social workers anticipating casualties among the agitating public, formed a voluntary street medic group. Initial formation was through a social media platform, calling for likeminded doctors and social workers to join the cause, finally amassed around 300 professionals, ready to be mobilized, under most trying circumstances.
Methods: The Case Study
The group had individual collections of first aid essentials, emergency drugs and consumables, stored into backpacks. They mingled among the agitating public, during mass protests, provided first aid, emergency care and coordinated with prehospital care ambulances for safe casualty retrieval and transport. Subsequently, as the sporadic street agitations moved to the Galle Face Green, together with Sarvodaya Movement, Sri Lanka Red Cross, and St. John’s, a field medical unit was formed at the site. A core-coordination group was formed to liaise with different stakeholders, formulate a roster for volunteer doctors, nurses and social workers, develop a mechanism for handling of donations and site safety including a mass casualty plan and an evacuation plan during emergency situations. Such were essential due to regular medical services could not approach the agitation site in their own right.
Afterwards, the basic unit was converted to a fully-fledged field medical unit with emergency facilities and four ambulances. Later, Psychological First Aid, routine medical clinics, dental and physiotherapy services were provided to resident agitators. Within a span of three months over 3000 patients and 450 patient transfers were handled. On 9th of July, the D Day, nearly 300 casualties were treated at the site.
Results
When conventional medical services are restricted, voluntary doctors can fill the vacuum for provision of essential emergency medical care for masses. However, principles of impartiality, neutrality, humanity, volunteerism along with highest standards of professionalism have to be maintained to prevent intrusions by vested parties to interrupt the services and discredit their genuine intentions and volunteerism.
Conclusions
This case highlights the rapid mobilization and coordinated efforts of street medics who, guided by principles of humanitarianism, provided continuity of essential medical care amidst civil unrest. It also demonstrated a scalable and community-based model of emergency response, which can be adapted for similar contexts of civil strife globally.

Exploring Loneliness and Social Isolation Among Emerging Adults in Kerala
Harigovind, Sree Chitra Tirunal Institute for Medical Sciences and Technology (SCTIMST), Thiruvananthapuram, India
Introduction: Background
Loneliness and social isolation have been recognised as a priority globally and endorsed by the World Health Organisation as a concern across all ages. While studies document this problem among older adults, emerging adults who face multiple challenges due to the transition to adulthood may experience newer problems in the current milieu of social media, personal aspirations and self-determination.
Objectives
This study aims to understand how emerging adults of the age group 18-29 years conceptualize loneliness and social isolation, the perceived causes, the coping mechanisms employed and the links between loneliness and social isolation.
Methods
The study used a qualitative mode of inquiry. Data collection techniques included a Free Association Grid Elaboration Method (GEM) and In-Depth Interviews (IDI). Twenty IDIs were conducted. Two Focus Group Discussions (FGD) were conducted to validate the findings. A hybrid coding approach was used to analyse the interviews and FGDs. The analysis was done using QualCoder version 3.5.
Results
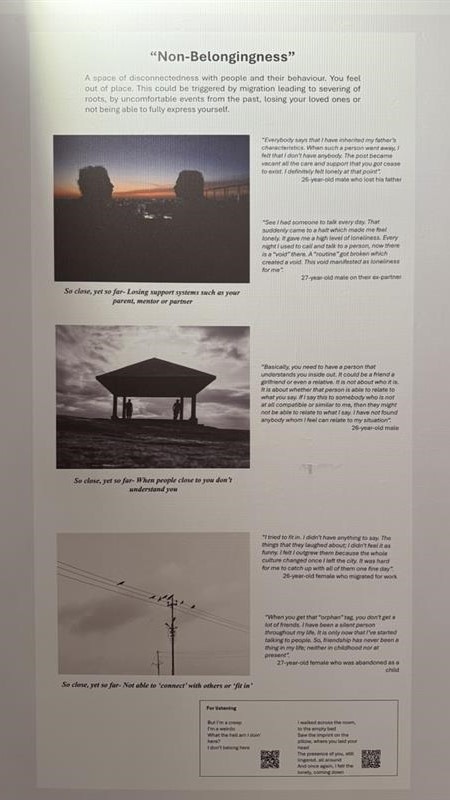
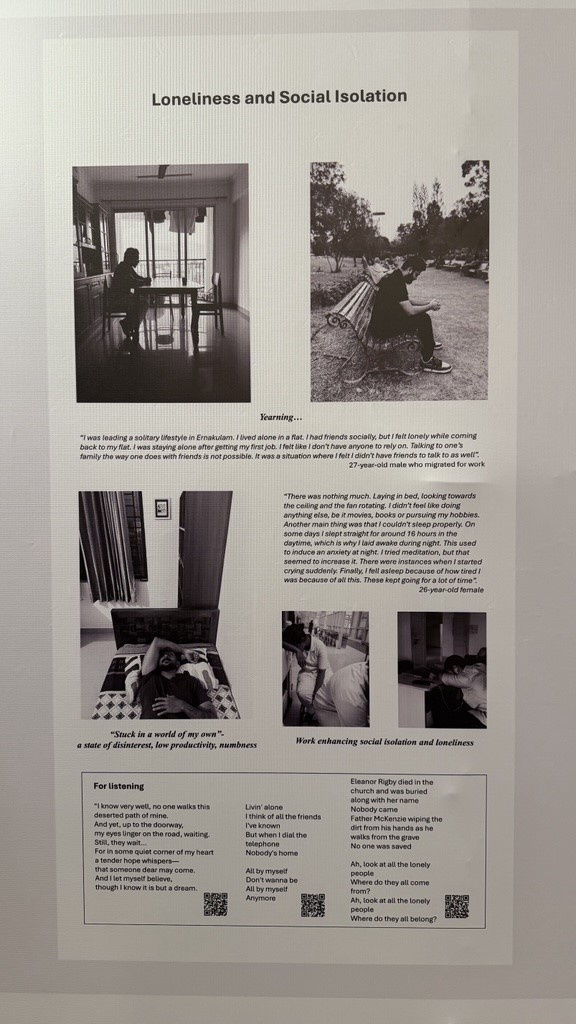
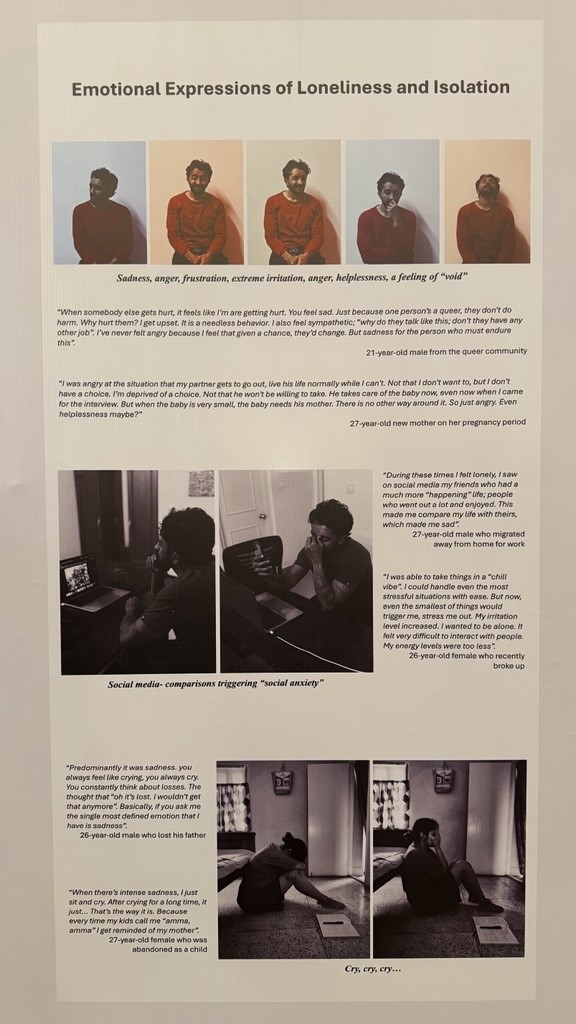
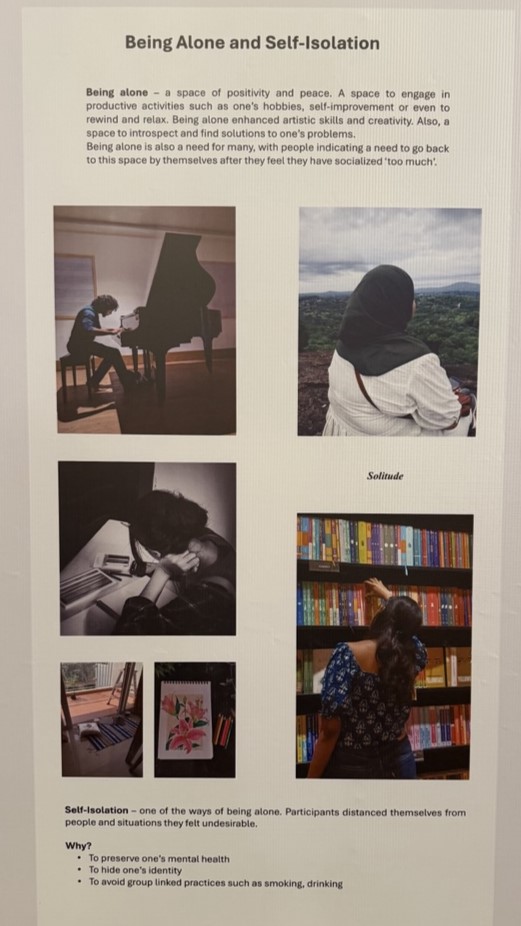
Conceptualizations of loneliness include non-belongingness, helplessness, duration, intensity and triggers for loneliness, and an identified difference from ‘being alone’. Sadness, anger, anxiety, restlessness, frustration, disappointment and guilt are the emotions associated with loneliness. Forms of social isolation included abandonment, pressurizing, ignoring, or emotional blackmailing. Both loneliness and social isolation were found to have negative consequences including a desperation to talk, insecurity, physical and emotional manifestations, self-harm, lingering trauma, substance abuse and developing hatred. Self-isolation was seen as a protective measure which included distancing or engaging in productive activities.
Reasons for loneliness and isolation included pregnancy and migration induced isolation, not belonging because of one’s identity, romantic breakups, loss of mentorship, not having people to talk to, financial distress and transitioning to adulthood and dealing with expectations. Reasons for self-isolation included preserving mental wellbeing, hiding identity, avoiding consequences of anger and avoiding group-linked practices like substance abuse. Coping mechanisms included external measures like seeking professional help, reaching out to similar groups or communities, venting frustration at partners, and internal measures like giving it time or crying.
Conclusions
Loneliness is an emotional state while social isolation is experienced by individuals due to actions of others and this is beyond their control. Both produce negative emotions and consequences. While individuals exhibit resilience in dealing with loneliness, the difficulty in managing social isolation is evidenced through idioms of distress. Self-isolation is different from social isolation and is a protective factor employed by emerging adults.
A Photovoice Exploration of Stigma in Women with Drug Resistant Tuberculosis in Mumbai
D. Jalgaonkar, TB Survivor Collective, Mumbai, India
Demo proposal
Drug-resistant tuberculosis (DR-TB) remains one of the world’s most serious infectious diseases, with stigma posing a significant barrier to its elimination—particularly among women in gender-inequitable settings. In India, the social consequences of DR-TB for women are profound yet insufficiently understood. This study sought to explore the lived experiences of stigma among women affected by DR-TB in Mumbai, focusing on the intersection of gender, health, and social marginalization. Using a participatory action research (PAR) approach with photovoice, nine women were invited to capture non-identifying photographs that reflected their personal experiences with stigma. Through group discussions, participants collectively interpreted 37 images and accompanying narratives, engaging in an iterative dialogue with each other and with researchers. This process offered rich, nuanced insights into the emotional and social dimensions of DR-TB stigma, as seen and articulated by those most directly impacted.
Proposed solution
By examining enacted, anticipated, and internalized stigma, participants revealed profound emotional and social consequences—including experiences of loss, abuse, and psychological distress. Yet, through the participatory process, women also began to reclaim their agency and foster resilience. Collective storytelling created a space for solidarity and healing, while enabling the development of shared strategies to resist stigma. These findings underscore the transformative potential of participatory, gender-sensitive approaches in reducing stigma, supporting mental well-being, and shaping more inclusive, compassionate models of TB care. The study highlights the urgent need to address gendered stigma within TB programs and demonstrates how centering the voices of affected women can drive more equitable and effective public health responses.
How a demo at a Scientific Days event will benefit your work
Presenting this work at the MSF Scientific Days—an event that brings together practitioners, researchers, and policymakers from diverse geographical and professional backgrounds—offers a critical opportunity to elevate the voices of marginalized communities and raise awareness about the pervasive stigma surrounding TB. We hope that sharing these insights on a global platform will not only deepen understanding but also inspire cross-country dialogue and action. By informing more compassionate and gender-sensitive policies, this work can contribute to reducing stigma and improving care for people living with TB worldwide.
Healing Through Humour: Evaluating the Impact of Medical Clowning on Patient Wellbeing in Indian Public Hospitals
Agarwal, Clownselors, Mumbai, India
Problem your innovation is addressing
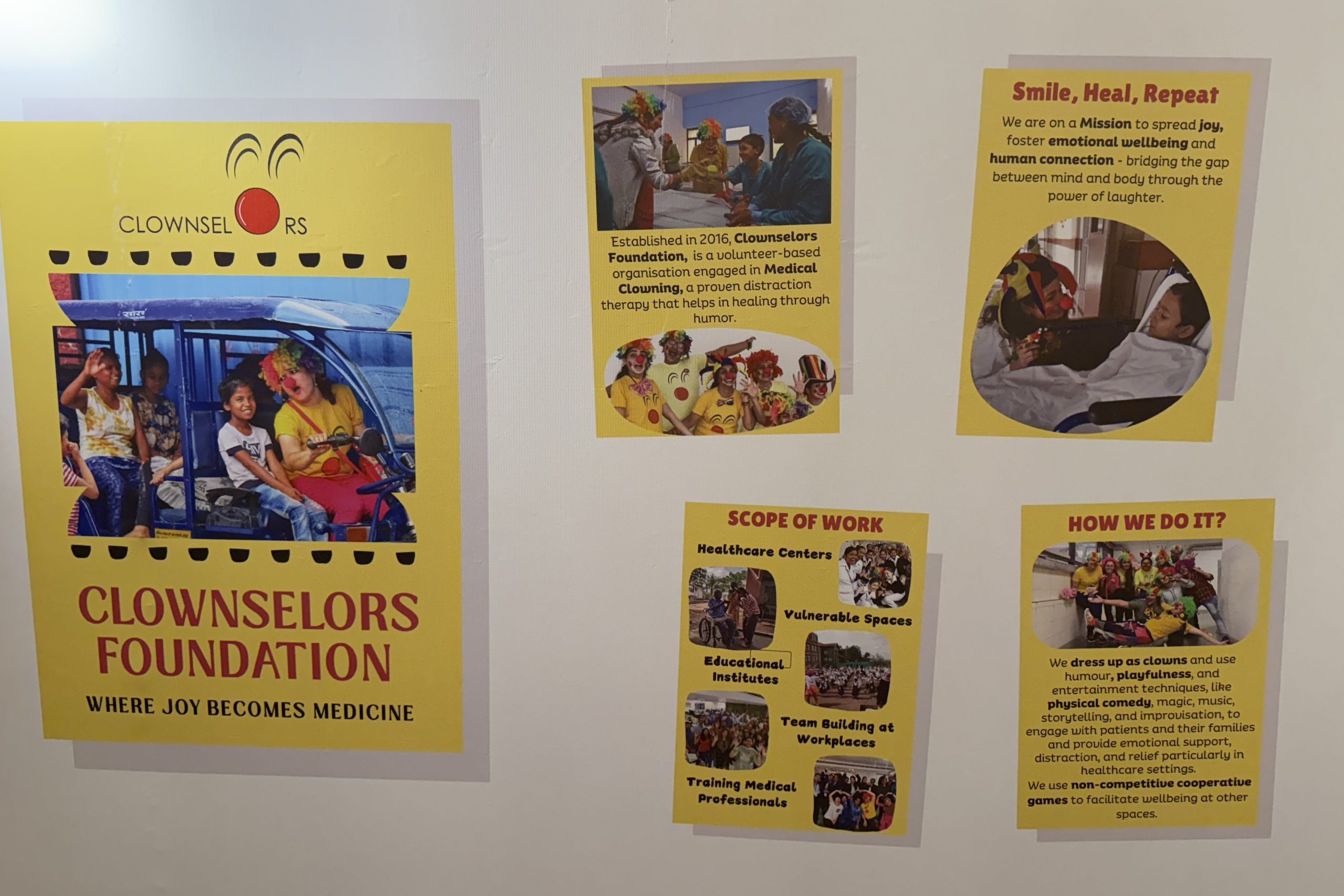
Psychosocial care is often sidelined in India’s resource-limited healthcare settings, despite its significance in patient recovery. Medical clowning, a therapeutic intervention using humor, play, and empathy, offers a low-cost, human-centered approach to address this gap.
Proposed solution
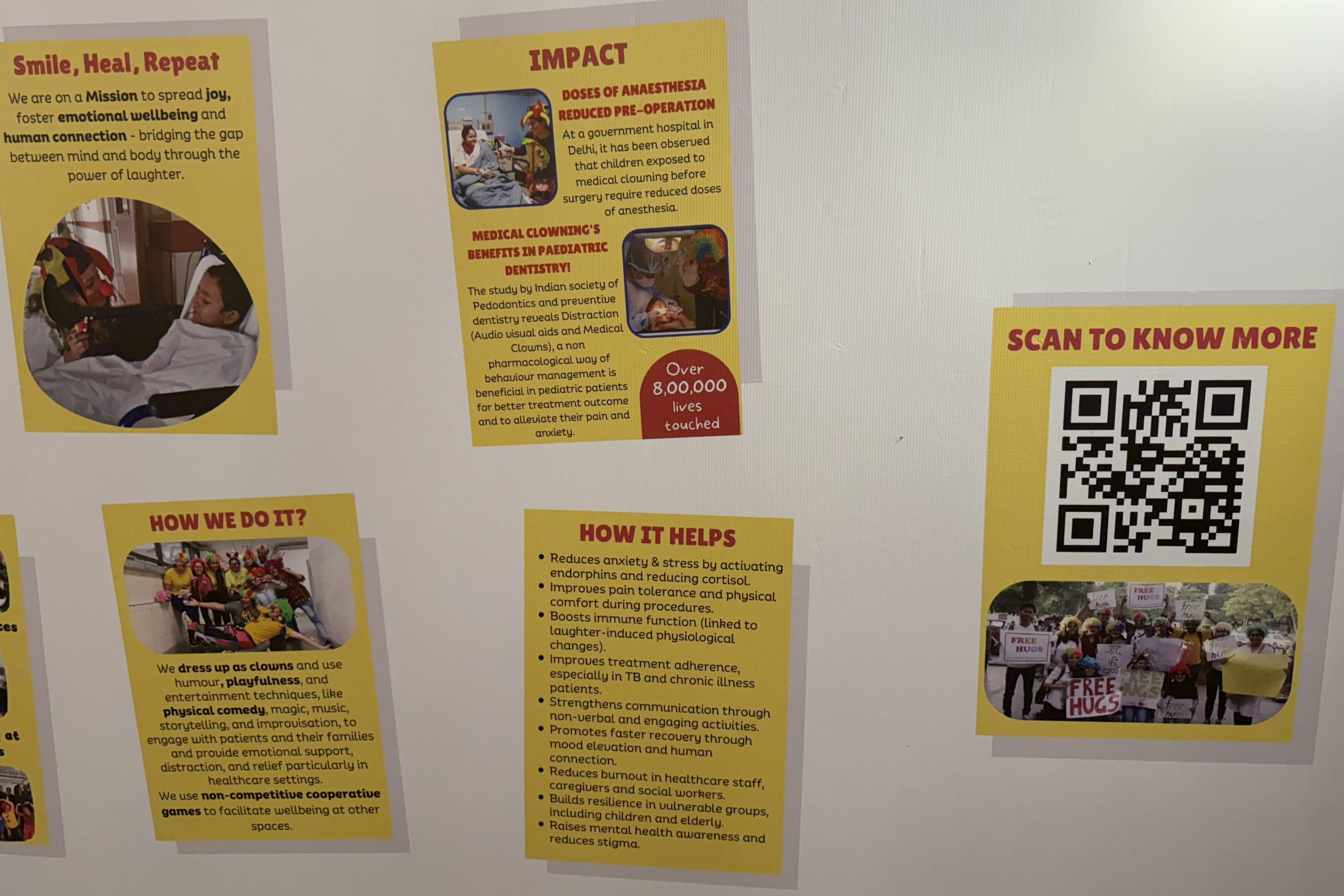
Across departments, clowning sessions visibly reduced patient anxiety and improved emotional responsiveness and cooperation. Pediatric wards reported decreased need for anxiolytics. In a TB OPD, at Shatabdi Hospital, Mumbai, patients became notably more communicative and engaged post-session. In oncology and palliative care, both patients and caregivers described the experience as uplifting and emotionally relieving, often referring to it as the “highlight” of their hospital stay.
Medical clowning proves to be a scalable and culturally adaptable psychosocial tool, enhancing patient experience and emotional resilience in clinical care. Its integration into routine health services could redefine the standard of compassionate care, making space for joy, connection, and dignity alongside treatment.
How a demo at a Scientific Days event will benefit your work
Presenting Clownselors’ work at Scientific Days allows us to share powerful, real-time experiences from hospital settings where humor and empathy ease distress. Our insights come not from numbers, but from genuine patient and caregiver responses, stories of fear turning into smiles. This platform offers a space for meaningful exchange, constructive feedback, and broader dialogue on compassionate care. We aim to highlight medical clowning as a low-cost, human-centered approach that deserves a place in India’s mainstream healthcare narrative. Where joy and dignity become integral to the healing process, not optional
“I have to put myself in their place”: Exploring empathy in humanitarian palliative care through stories from Cox’s Bazar, Bangladesh
Yantzi, MSF, Barcelona, Spain and McMaster University, Hamilton, Canada
Introduction
Consistent with MSF’s strategic focus on person-centered care, palliative care has been increasingly recognized as a priority. At the MSF Goyalmara Mother-Child Hospital in Cox’s Bazar, Bangladesh, efforts have been made to integrate palliative care due to high mortality and medical complexity of patients. The aim of this study is to explore the meaning of empathy to international and locally hired MSF staff at Goyalmara Hospital, and their moral experiences of attempting to provide empathetic palliative care.
Methods
This focused ethnography was conducted between March-August 2021 at Goyalmara Hospital. Data collection involved participant-observation, individual interviews (22), and focus group discussions (5). Interviews and focus groups were audio-recorded, translated, and transcribed. A coding scheme was developed, and data coded using NVivo 11. Researchers reviewed all data that had been coded as “sympathy and empathy” as well as related codes, while considering analytic questions developed based on the literature. Researchers engaged in analytic discussions, memo-writing, and mind-mapping exercises to develop themes. Then composite stories were written based on situations described in field notes, incorporating quotations from interviews and focus groups in order to explore themes emerging from the analysis.
Results
Empathy, as well as related Bangla concepts of maya, shohanubhuti and shohomormita, were central to how MSF staff understood good palliative care. These concepts informed how MSF staff experienced their relationships with the children and caregivers receiving palliative care, yet staff struggled to both express and maintain empathy over time. Using three composite stories, we explore how MSF staff’s values related to empathy were realized and thwarted in their everyday work while providing palliative and end of life care at Goyalmara Hospital.
Conclusions
MSF staff saw empathy as important in their interactions with patients and families receiving palliative and described profound experiences of connection. However, their values related to empathy were often challenged as they struggled to maintain a distinction between their own experiences and those of their patients and families. Other staff worried that they were “becoming a mechanical person” due to their frequent exposure to loss and death.
Empathy is essential given the heightened moral complexity of humanitarian palliative care. It is critical that capacities related to empathy are developed in humanitarian healthcare workers.